
I. Introduction
The use of an automated external defibrillator (AED) in out of hospital cardiac arrests (OHCAs) is pivotal in improving outcomesfor patients [1-5]. This is an issue of major concern due to the increasing prevalence of cardiac arrests in Singapore, and the high mortality rates of OHCAs [6]. Then umber of OHCAs has increased from 2503 in 2016 to 2972 in 2018 and is likely to increase further due to the aging population in Singapore. Additionally, the current bystander AED usage is 7.2% of OHCAs [6]. Arecent study of AED usage in European countries shows that better AED usage rates of 25% to 58% are attainable [7]. Hence, it is of great importance to identify and reduce barriers to AED use in the community. In Korea, the OHCA rate is 66.7 per 100,000 [8]. However, bystander AED use remains low at around 0.13% [9], with a Korean study finding that 65% of participants did not know how to use an AED [10].
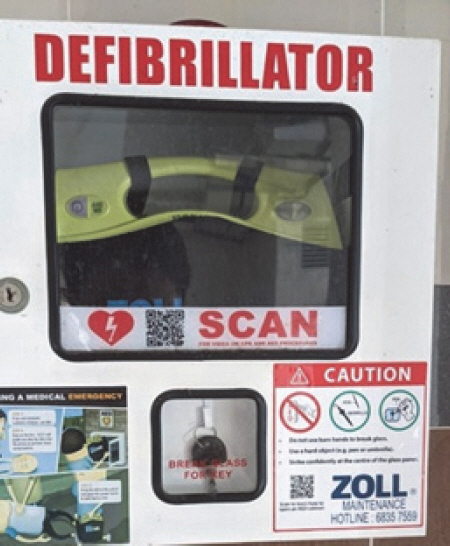
Public access AEDs in Singapore are secured in a locked box, with the key to the box secured behind a pane of glass <Fig. 1>. Occasionally, members of the public have been injured while retrieving AEDs during OHCAs <Fig. 2>, such as by being cut by glass while breaking the pane of glass or retrieving the key [11]. Public access AEDs are commonly found at public housing estates, schools, sports facilities, transportation hubs, government buildings and most commercial premises.
Fig. 1
A typical AED box found at a housing estate in Singapore. Note that the graphic on the box demonstrating how to break the glass safely was only recently added.

Factors affecting AED retrieval include the AED retrieval distance, which is the distance a responder must travel to the nearest available AED, and the time of day that retrieval is attempted. Studies [12] have shown that a larger AED retrieval distance is correlated with decreased survival. Other studies in Britain [13] and Denmark [14] have shown that only a third, and less than half of AEDs, respectively, were available at night, due to being placed in areas such as offices, school facilities or clinics.
Prior work on integrating technology and AED retrieval has mainly explored methods to aid AED retrieval, but with mixed results. A study [15] trialled a Mobile AED map to improve access to AEDs -which was unable to shorten AED retrieval time. A more recent simulation [16] assessing a mobile Geolocalization application in locating AEDs found that it was of no aid at all in locating AEDs. Research on novel methods to optimize AED retrieval have mainly focused on drone delivery of AEDs to OHCA sites. Studies [17,18] have shown that drone delivery of AEDs to an incident site can result in more rapid retrieval than physically retrieving an AED.
Despite the prior work done on optimizing AED retrieval and variables affecting AED retrieval, there is a research gap in terms of examining the safety of AED retrieval. This break glass cabinet is unique to few countries, hence the safety of this retrieval mechanism has not been previously studied. This study addresses a knowledge gap by attempting to quantify how common injuries are among community responders in Singapore.
This study aims to elucidate predictive factors influencing successful retrieval of an AED, as well as document the prevalence of injuries among community responders, and factors affecting responders’ willingness to respond to cardiac arrest cases in the future.
II. Methods
1. Study design
As there was no published peer review research in this area, we reached out to more established AED registries in Denmark and Australia to inquire about injuries related to AED retrieval. We searched online for local news report and reached out to the Singapore Civil Defence Force and AED manufacturers. Focus group interviews were also conducted with experienced first responders and emergency physicians to design a pilot survey that was tested iteratively with the investigators followed by volunteers to develop the final survey that was used in the study. The phrasing and variables suggested to be critical in predicting success of AED retrieval were derived through this multi-stage process of survey design.
These variables include responder factors, such as age, gender, and occupation. These factors were chosen as they are simple demographic data which may affect the success of retrieving an AED. Environmental factors included AED retrieval distance and time of day as these were shown to be significant in prior work on success or speed of AED retrieval.
2. Data collection
The online survey form was created with the use of a secure survey portal launched by the Government Technology Agency of Singapore called FormSG. The survey was circulated via a Facebook group set up by the SCDF to engage online with Community First Responders, many of whom use the myResponder app. The survey link was also sent to First Aid Training Centres and local First Aid Organizations such as Singapore Red Cross and St John Singapore. The survey was disseminated to these groups as it was likely that these individuals would have attempted to retrieve an AED before. The data collection period was from 1st Jan 2021 to 1st Mar 2021. The respondents should have responded to a cardiac arrest in the previous 12 months.
The survey included questions on the participant’s demographics such as age, occupation and whether they had undergone AED training before. In addition, targeted questions were asked about their previous experiences while responding to an OHCA, including whether participants had ever been injured while retrieving an AED, and if so, the site of the injury and what treatment was required. Finally, participants were asked to share suggestions for possible improvements to AED retrieval.
Participants who were surveyed were informed that their participation was voluntary and could be terminated at any point. In addition, no personally identifying information was collected.
3. Inclusion and exclusion criteria
To be included in the study, participants must have responded to a OHCA in the past 12 months. Participants who did not respond to an OHCA within the past 12 months were excluded from the survey. As the online survey form prevented these participants from submitting the survey if they did not meet the inclusion criteria, the number of these participants was not collected. The participants were then split into two groups - those who had attempted to retrieve an AED and those who had not. Successful retrieval of an AED would include retrieving an AED and bringing it to the casualty suffering from cardiac arrest.
4. Data analysis
Categorical data was expressed in frequency and percentage. Comparison tests were performed with Fischer-Freeman-Halton Exact test if there were at least 1 cell count <5 and otherwise, Pearson chi square test at 5% significance levels. Data analysis was done by using IBM® SPSS® Statistics version 25 software.
The statistical analysis for inferring the success of AED retrieval of odds ratio (OR) was conducted using multiple logistic regression with a logit link function. Based on our literature review and communication with responders and subject matter experts, we selected variables commonly known to be associated with OHCA survival. We postulated in addition factors that may predict success of AED retrieval, such as age, gender, occupation and time of day.
III. Results
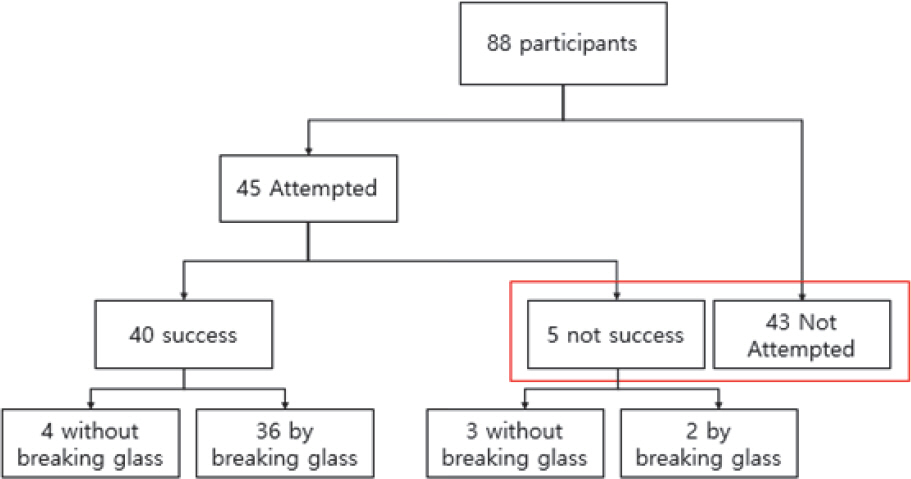
Excluding those who had never responded to a cardiac arrest, and those who did so more than 12 months ago, 88 participants responded to the survey. As shown in <Fig. 3>, of 88 participants, 45 attempted retrieval and 43 participants did not. Of the 45 whom attempted retrieval, 40 succeeded while 5 failed.
Fig. 3
Flowchart showing of participants. Participants enclosed by the red box are grouped as “Not successful”in retrieving an AED.
Demographic data of the participants is represented in <Table 1>. Most responders tend to be male (75.0%), with the most common age of responders being from 21-25 years old, for both males (30.0%) and females (31.3%). The oldest responder was in the 61-65 year age group, while 10 responders were aged 16-20, making up 11.4% of all the survey participants. Almost all the participants had received AED training in their lifetime, with only 1 participant (1.1%) never having undergone training. 46 (52.3%) respondents were healthcare professionals, including doctors, nurses, paramedics, medics, allied healthcare staff and healthcare students.
Table 1
Demographic data of the survey participants
| Successful in retrieving AED† (n = 40) | Not Successful in retrieving AED (n = 48) | P value‡ | |
|---|---|---|---|
| Gender, n (%) | 0.642 | ||
|
|
|||
| Male | 30 (75.0%) | 35 (72.9%) | |
|
|
|||
| Female | 10 (25.0%) | 13 (27.1%) | |
|
|
|||
| Age group, n (%) | 0.314 | ||
|
|
|||
| 16-20 | 6 (15.0%) | 4 (8.3%) | |
|
|
|||
| 21-25 | 12 (30.0%) | 15 (31.3%) | |
|
|
|||
| 26-30 | 5 (12.5%) | 5 (10.4%) | |
|
|
|||
| 31-35 | 9 (22.5%) | 7 (14.6%) | |
|
|
|||
| 36-40 | 1 (2.5%) | 4 (8.3%) | |
|
|
|||
| 41-65 | 7 (17.5%) | 13 (27.1%) | |
|
|
|||
| Occupation, n (%) | 0.940 | ||
|
|
|||
| Nurse | 8 (20.0%) | 10 (20.8%) | |
|
|
|||
| Doctor | 1 (2.5%) | 1 (2.1%) | |
|
|
|||
| Paramedic/Medic | 8 (20.0%) | 11 (22.9%) | |
|
|
|||
| Others | 23 (57.5%) | 26 (54.2%) | |
|
|
|||
| Previous Training Experience, n (%) | 1.000 | ||
|
|
|||
| Received Training | 40 (100.0%) | 47 (97.9%) | |
|
|
|||
| Never Received Training | 0 (0.0%) | 1 (2.1%) | |
As shown in <Table 2>, from the result of the Pearson Chi square test and Fischer’s exact test we found that the success of retrieving an AED is not impacted by occupation, age, nor gender. In addition, the success of retrieving an AED was not impacted by the time of day that retrieval was attempted. However, the method of breaking glass and injuries while retrieving AEDs was shown to be significant (p<.001).
Table 2
Data on the incidents which survey participants responded to
| Successful in retrieving AED† (n = 40) | Not Successful in retrieving AED* (n = 48) | P value‡ | |
|---|---|---|---|
| Time of Response to Incident, n (%) | 0.938 | ||
|
|
|||
| Day (7am-7pm) | 26 (65.0%) | 32 (66.7%) | |
|
|
|||
| Night (7pm-7-am) | 13 (32.5%) | 14 (29.2%) | |
|
|
|||
| Unsure | 1 (2.5%) | 2 (4.2%) | |
|
|
|||
| Mode of Activation, n (%) | 0.004 | ||
|
|
|||
| myResponder App | 38 (95.0%) | 34 (70.8%) | |
|
|
|||
| Others | 2 (5.0%) | 14 (29.2%) | |
|
|
|||
| Attempted to retrieve AED, n (%) | 1.000 | ||
|
|
|||
| Attempted | 40 (100.0%) | 5 (10.4%) | |
|
|
|||
| Did not Attempt | 0 (0.0%) | 43 (89.6%) | |
|
|
|||
| Reasons for not retrieving AED§, n (%) | |||
|
|
|||
| Was already performing CPR | NA | 19 (39.6%) | |
|
|
|||
| AED was not within sight | NA | 14 (29.2%) | |
|
|
|||
| SCDF had arrived | NA | 11 (22.9%) | |
|
|
|||
| Other‖ | NA | 43 (89.6%) | |
|
|
|||
| Injured while retrieving AED, n (%) | <0.001 | ||
|
|
|||
| Injured | 22 (55.0%) | 2 (4.2%) | |
|
|
|||
| Not Injured | 18 (45.0%) | 3 (6.3%) | |
|
|
|||
| Not Applicable | 0 (0.0%) | 43 (89.6%) | |
|
|
|||
| Method of Breaking Glass¶ | <0.001 | ||
|
|
|||
| Using items only | 22 (61.1%) | 1 (2.08%) | |
|
|
|||
| Using body parts | 14 (38.9%) | 1 (2.08%) | |
|
|
|||
| Not Applicable | 4 (10.0%) | 46 (95.8%) | |
† Participants who were successful in retrieving an AED were able to remove it from the AED cabinet and bring it to the scene of the cardiac arrest
§ Top 3 Reasons for not retrieving AED: Participants were able to state multiple reasons for not retrieving an AED
<Table 3> shows that participants who used their body parts to break glass were found to be significantly more likely to injure themselves compared to participants who used items to break the glass. 38 participants attempted to break glass, of whom 2 failed and 36 succeeded. Of these 38 participants, 24 were injured (63.2%). However, as shown in <Table 2>, regardless of whether items or body parts were used, there was no significant difference in success of retrieving AEDs.
Table 3
Data table of injuries and method of breaking glass†
| Injured (n = 24) | Not injured (n = 14) | Total (n=38) | |
|---|---|---|---|
| Method of Breaking Class, n (%)† | |||
|
|
|||
| Using Items only | 9 (37.5%) | 14 (100.0%) | 23 (60.5%) |
|
|
|||
| Using body parts | 15 (62.5%) | 0 (0.0%) | 15 (39.5%) |
<Table 4> shows that being injured while responding to an OHCA did not make responders less willing to retrieve an AED in future. Of the 24 respondents who sustained injuries from breaking glass, only 1 (4.17%) reported being unwilling to retrieve an AED in future, with 17 (70.8%) continuing to be very willing to retrieve an AED in future. Two responders who lost or damaged personal items while responding also reported their willingness to retrieve an AED in future as very willing to do so.
Table 4
Data table of willingness to retrieve AED in future†
| Injured (n = 24) | Not injured (n = 14) | Total (n=38) | |
|---|---|---|---|
| Willingness to retrieve AED in future† | |||
|
|
|||
| Very willing | 17 (70.8%) | 11 (78.6%) | 28 (73.7%) |
|
|
|||
| Willing | 2 (8.3%) | 0 (0.0%) | 2 (5.3%) |
|
|
|||
| No difference | 4 (16.7%) | 3 (21.4%) | 7 (18.4%) |
|
|
|||
| Unwilling | 1 (4.17%) | 0 (0.0%) | 1 (2.6%) |
|
|
|||
| Very unwilling | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
Participants who responded to an OHCA because of activation by the myResponder App were found to be more likely to retrieve an AED successfully. The univariate and multivariate odds ratio of retrieving an AED successfully increase greatly for individuals who are activated through the myResponder App. (OR 4.5) (AOR 11.111, 95% CI: 2.141-58.824) <Table 5><Table 6>
Table 5
The univariate logistic regression demonstrating that activation via myResponder app increases the odds of retrieving an AED
| Variables | n (%) | Coefficient | Wald | P-value | Odds ratio (95% CI) |
|---|---|---|---|---|---|
| Time | |||||
|
|
|||||
| Day (7am-7pm) (ref) | 58 (65.8) | 1.000 | |||
|
|
|||||
| Night (7pm-7-am) | 27 (30.7) | -0.762 | 0.370 | 0.543 | 0.467 (0.040-5.435) |
|
|
|||||
| Unsure | 3 (3.4) | -0.767 | 0.357 | 0.550 | 0.464 (0.037-5.749) |
|
|
|||||
| Mode of Activation. | |||||
|
|
|||||
| Others* (ref) | 16 (18.2) | 1.000 | |||
|
|
|||||
| myResponder App | 72 (81.8) | 2.444 | 9.546 | 0.002 | 11.518 (2.444-54.281) |
|
|
|||||
| Gender | |||||
|
|
|||||
| Male (ref) | 65 (73.9) | 1.000 | |||
|
|
|||||
| Female | 23 (26.1) | 0.056 | 0.013 | 0.908 | 1.058 (0.408-2.740) |
|
|
|||||
| Age (years) | |||||
|
|
|||||
| 16-20 (ref) | 10 (11.4) | 1.000 | |||
|
|
|||||
| 21-25 | 27 (30.7) | -1.466 | 3.089 | 0.079 | 0.231 (0.045-1.184) |
|
|
|||||
| 26-30 | 10 (11.4) | -0.842 | 1.918 | 0.166 | 0.431 (0.131-1.419) |
|
|
|||||
| 31-35 | 16 (18.2) | -0.619 | 0.618 | 0.432 | 0.538 (0.115-2.519) |
|
|
|||||
| 36-40 | 5 (5.7) | -1.130 | 2.624 | 0.105 | 0.323 (0.082-1.268) |
|
|
|||||
| 41-65 | 20 (22.7) | 0.767 | 0.401 | 0.527 | 2.154 (0.200-23.183) |
|
|
|||||
| Occupation | |||||
|
|
|||||
| Nurse (ref) | 18 (20.5) | 1.000 | |||
|
|
|||||
| Doctor | 2 (2.7) | 0.041 | 0.005 | 0.941 | 1.042 (0.354-3.069) |
|
|
|||||
| Paramedic/Medic | 19 (21.6) | 0.041 | 0.001 | 0.977 | 1.042 (0.062-17.613) |
|
|
|||||
| Others | 49 (55.7) | -0.065 | 0.014 | 0.905 | 0.938 (0.325-2.707) |
Table 6
The Multivariate logistic regression demonstrating that activation via myResponder app increases the odds of retrieving an AED
| Variables | n (%) | Coefficient | Wald | p value | Odds ratio (95% CI) |
|---|---|---|---|---|---|
| Time | |||||
|
|
|||||
| Day (7am-7pm) (ref) | 58 (65.8) | 1.000 | |||
|
|
|||||
| Night (7pm-7-am) | 27 (30.7) | 0.584 | 0.127 | 0.722 | 1.793 (0.072-44.666) |
|
|
|||||
| Unsure | 3 (3.4) | 0.487 | 0.090 | 0.764 | 1.627 (0.068-38.993) |
|
|
|||||
| Mode of Activation. | |||||
|
|
|||||
| Others* (ref) | 16 (18.2) | 1.000 | |||
|
|
|||||
| myResponder App | 72 (81.8) | 2.406 | 8.226 | 0.004 | 11.111 (2.141-58.824) |
|
|
|||||
| Gender | |||||
|
|
|||||
| Male (ref) | 65 (73.9) | 1.000 | |||
|
|
|||||
| Female | 23 (26.1) | 0.401 | 0.216 | 0.642 | 1.493 (0.275-8.096) |
|
|
|||||
| Age (years) | |||||
|
|
|||||
| 16-20 (ref) | 10 (11.4) | 1.000 | |||
|
|
|||||
| 21-25 | 27 (30.7) | -1.759 | 1.324 | 0.184 | 0.013 (0.013-2.307) |
|
|
|||||
| 26-30 | 10 (11.4) | -1.707 | 0.853 | 0.045 | 0.181 (0.034-0.965) |
|
|
|||||
| 31-35 | 16 (18.2) | -2.134 | 1.290 | 0.098 | 0.12 (0.01-1.48) |
|
|
|||||
| 36-40 | 5 (5.7) | -1.321 | 1.003 | 0.188 | 0.267 (0.037-1.906) |
|
|
|||||
| 41-65 | 20 (22.7) | -0.384 | 1.189 | 0.747 | 0.681 (0.066-7.002) |
|
|
|||||
| Occupation | |||||
|
|
|||||
| Nurse (ref) | 18 (20.5) | 1.000 | |||
|
|
|||||
| Doctor | 2 (2.7) | -0.236 | 0.710 | 0.790 | 0.790 (0.139-4.491) |
|
|
|||||
| Paramedic/Medic | 19 (21.6) | -20.483 | 0.000 | 0.999 | 0.000 (0.000-0.000) |
|
|
|||||
| Others | 49 (55.7) | -0.560 | 0.383 | 0.536 | 0.571 (0.097-3.367) |
IV. Discussion
This is an unprecedented study done to understand the challenges of retrieving public access AEDs and the risks of injury to responders while retrieving the devices, as this mechanism is unique to only a few countries including Singapore. In addition, this is the first time that community responders have been surveyed to find out their demographics, and the challenges they face while responding to cardiac arrests in the community. This is because there is no registry of responders, and these responders are not always known to Emergency Medical Services, so it is challenging to perform a survey of this population.
This break glass method of securing AEDs is uncommon. We have contacted AED manufacturers and emailed resuscitation researchers in USA, Europe and Asia to ask about break glass mechanisms. Of the countries which the AED manufacturer supplies, only Malaysia locks their AEDs in a similar manner to Singapore while neighbouring countries such as Indonesia, Philippines and Vietnam, have their AEDs locked up with the keys being kept with the building management [19]. In other countries such as Denmark, Thailand, Indonesia and Hong Kong, AEDs are usually left unlocked, or secured with a passcode provided by EMS dispatchers [20]. As such, little is known whether this method of securing the AED prevents responders from successfully retrieving an AED, as well as the prevalence of injuries among community responders.
To improve the bystander CPR and defibrillation rates, the Singapore Civil Defence Force (SCDF) launched the myResponder mobile application in 2015, which harnesses GPS geolocation to inform users when someone in their vicinity is suffering from a suspected cardiac arrest. Emergency dispatchers can trigger the app to activate nearby community responders. Notwithstanding, the app also provides responders with a map of nearby AEDs to facilitate retrieval of an AED. The use of the myResponder app has helped to crowdsource trained volunteers and has likely been one of many factors which helped to increase the number of AEDs brought to scene of cardiac arrest cases in Singapore [21]. The rate of bystander AED use increased from 4.0% of OHCAs in 2015 to 7.2% of OHCAs in 2018.
The results of this study are encouraging as they reveal that members of the public remain equally motivated to retrieve an AED despite being injured in the process, with only 3.4% of respondents being less willing to retrieve an AED in future due to injuries sustained. Participants who were injured reported injuries such as cuts in places such as their fingers, palms or knuckles. In addition, all survey participants who sustained injuries were able to treat the injuries at home, with none going to a clinic or hospital for medical treatment, suggesting that the injuries are likely to be minor. The study also shows that responders remain motivated to respond to OHCAs despite facing challenges such as injuries or losing personal items, as there was no significant difference in willingness to retrieve AEDs in future, for both injured and uninjured responders. This highlights that community responders are motivated to help in OHCAs. However, only four individuals lost or damaged items while responding, so the attitudes of these four individuals may not be generalizable to all responders.
Furthermore, the data collected from this study suggests that the myResponder App helps to improve the response to OHCAs. This is consistent with other studies which show that mobile applications are able to facilitate CPR and early defibrillation[22,23]. 77.3% of the study participants responded to a cardiac arrest case after being activated by the myResponder app. Participants who responded after being activated by the myResponder App were 11.1 times more likely to retrieve an AED than responders who witnessed the collapse or were notified by other means. This could be because the myResponder App simplifies information flow by alerting users of the AEDs, providing a detailed map showing the location, facilitating retrieval by the responder. Alternatively, it is also plausible that the community responders using the myResponder app are often more experienced and better prepared to retrieve AEDs.
Other demographic data collected from the survey also show that both men and women, regardless of age, are equally likely to succeed in retrieving an AED. The success in retrieving an AED is also independent of the participant’s occupation; non-healthcare professionals are as likely to succeed in retrieving an AED as paramedics or healthcare professionals, suggesting that the AED are designed adequately for laypersons to utilise. This data shows that many participants across age, gender and occupation can retrieve an AED, should they need to.
Success in retrieving an AED is also independent of the time of day, with participants retrieving AED with similar success rates in the day or at night. This is in contrast with other studies in Denmark and London, which show that AEDs are more difficult to retrieve at night and in the evening[13,14]. The increased accessibility of AEDs in Singapore at night might be due to a combination of factors, including the locations they are placed, how they are secured, and clear labelling and signage. As mentioned earlier in this paper, AEDs in other countries are often secured by keys held by the building management or security staff. Hence, this may show that the break glass cabinets allow access to AEDs regardless of the time of day.
V. Limitations and Future work
Our study has some limitations. Firstly, the participants of this study were sourced from a Facebook group containing community responders who had downloaded the myResponder App, and from First Aid Training Centres and First Aid societies. The sample size of 88 participants is also small. Hence, this study may not be completely generalizable to the population at large. This population was chosen as a survey done on the general population might contain very few eligible participants. Thus, there is room for further study, with a larger population or a longer study period, before conclusions can be made in terms of how successfully laymen can succeed in retrieving an AED.
While this study shows that community responders who sustain injuries were not deterred from responding in future, more research is required to devise better ways to secure the AEDs yet allowing responders to retrieve AEDs successfully, efficiently and safely during a cardiac arrest event.
Another area where further study is warranted is studying the functions of the myResponder app which users find most helpful in aiding them to retrieve an AED successfully. In this study, users who used the app were classified together, without considering which functions of the app they used the most, or at all. The app includes multiple features, including an AED map and a dispatcher-triggered alert to nearby OHCAs. Further study could identify specific features of the app which aided responders and improve the understanding of variables affecting AED retrieval.
VI. Conclusion
In conclusion, this novel study has increased our understanding of the demographics of community responders in Singapore, as well as the challenges they face and the factors affecting success of AED retrieval. Responders are significantly more likely to retrieve an AED without personal injury if they use an object to break the glass rather than a part of their body. The use of an object to break glass is just as effective in AED retrieval as using one’s hands, suggesting that responders would benefit from using available objects to break glass. The use of myResponder mobile application is associated with a much greater likelihood of successfully retrieving an AED. Successful retrieval of AED is not impacted by the time of day that retrieval is attempted, nor by the gender, age or occupation of the person attempting to retrieve the AED.




